
HCMC Math: The Numbers
We all have an HCMC connection. Maybe you were born there. Maybe your friend’s first job was there. Maybe your cousin received life-saving care there. HCMC does not turn anyone away. No matter who you are, whether you have insurance, or how you arrive at its doors — HCMC will care for you. That mission is what makes HCMC irreplaceable, and it is also what makes the finances so structurally difficult.
On April 23, 2026, Hennepin County staff presented a detailed financial briefing to the Board of Commissioners and the public on the severity of what HCMC faces. The presentation was clear: without a permanent, dedicated source of revenue, HCMC cannot remain open. This is not a crisis that appeared overnight, and it cannot be solved by a single infusion of cash or another property tax increase. HCMC needs a runway to make organized, strategic changes from a position of stability rather than collapse; its mission is essential for the health and well-being of all Minnesotans.
HCMC is the only public safety-net hospital in the Upper Midwest
HCMC has no significant reserves due to being a county-owned hospital, no investment earnings like other health systems, and therefore no cushion to absorb financial shocks that are affecting all hospitals and clinics. Every systemic change in revenue lands directly on the hospital's ability to operate.
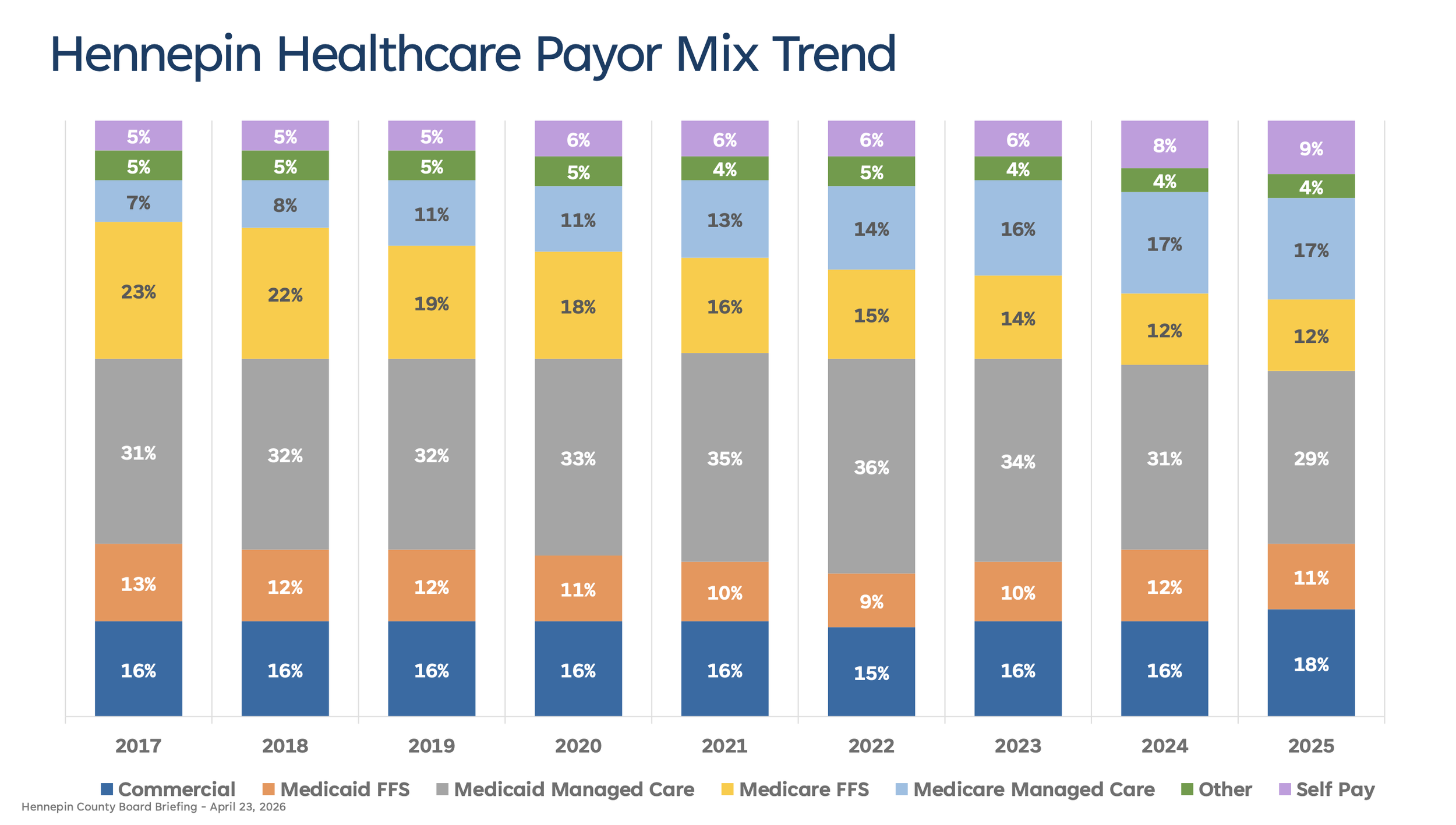
75% of HCMC patients pay using public programs like Medicaid and Medicare. When combined with self-pay patients, and over 80% of HCMC patients have no payment method that covers the full cost of their care.
Public programs do not reimburse at the full cost of care — in other words, we make up the financial gap in order to serve our mission and care for the most vulnerable.
Public programs generally reimburse at a much lower rate than commercial insurance — in other words, we make up the financial gap in order to serve our mission and care for the most vulnerable.
~24% of uncompensated care costs in 2024 were from serving patients who live outside Hennepin County — HCMC is a statewide resource and Hennepin property taxpayers funded 37% of uncompensated care in 2024.
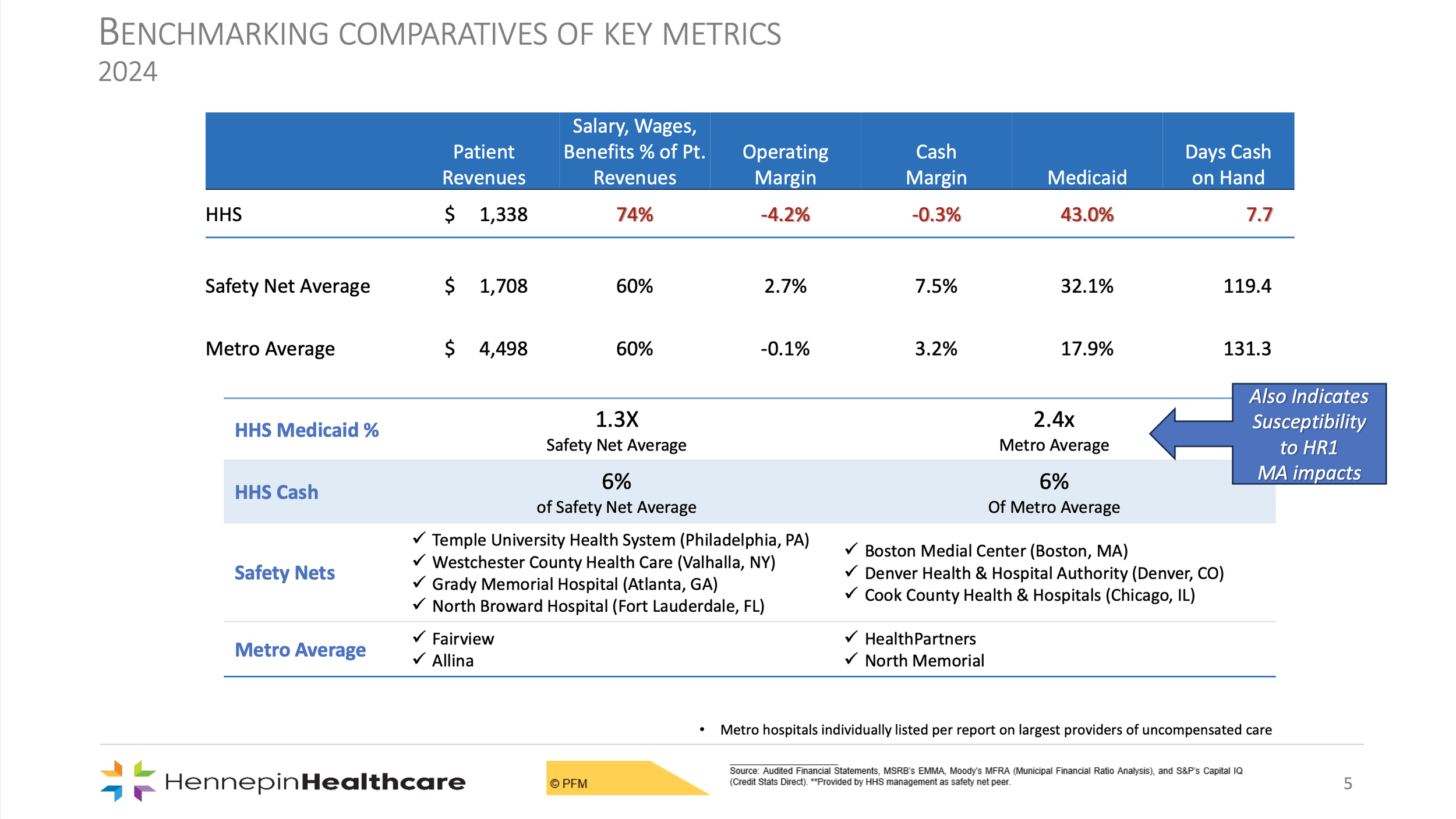
HCMC had 7 days cash on hand in 2024 (compared to 131 days on average for metro hospitals), and had a negative cash balance for several weeks in 2026.
It is meaningful to note for the image below — 2024 numbers are the most recent data to compare, most hospitals are not peers as public safety-nets, and several hospitals have had major ownership announcements since 2024.
HCMC is unique because of who we serve
It’s important to look at how HCMC compares to safety-net hospitals nationally and to other metro health systems in Minnesota to see the scale of the challenge.
HCMC's percentage of Medicaid patients is more than double the rate at most other metro hospitals in Minnesota and is significantly higher than the national safety-net average. This is not a gap that can be managed through operational efficiency alone; it is a structural feature of what it means to be the public option of last resort.
Because HCMC's revenue is so constrained by its payor mix — salaries, wages, and benefits represent a higher percentage of revenue than at peer institutions. This does not mean that HCMC overspends on labor, it just means that our revenue ratio is much smaller than other MN hospitals. This distinction matters when Hennepin County is asked why costs can't simply be cut.
Budget Crisis and How We Got Here
The structural financial pressures HCMC faces have been building for years, but several specific events accelerated the crisis and left the hospital with no cushion to absorb what came next.
A significant recent blow was the dissolution of UCare, which had been HCMC's largest insurance payor. UCare, a nonprofit health plan, abruptly shut down its operations at the end of 2025 (a few months after the County Board resumed interim oversight), leaving HCMC with further debt. For a hospital already operating with 7 days of cash on hand, the loss of its largest payor was significantly difficult.
At the same time, the Medicaid presumptive eligibility ended in 2023 and pushed thousands of Minnesotans off insurance coverage across the state. This means more patients arrive at HCMC without any coverage at all, raising uncompensated care costs significantly.
These shocks arrived at a hospital that had no reserves to absorb them — and they are the direct reason the County Board intervened in August 2025 to serve as HCMC's interim board and keep the hospital open. Numerous other hospitals and clinics in Minnesota and nationally were unable to absorb these financial shocks — which has resulted in a record number of closures, mergers, sales, and bankruptcy filings.
Structural deficits HCMC faces even before accounting for federal changes (growing expenses)
All of this is before the impacts of HR1 are felt. Because of its disproportionate Medicaid population, HCMC will be hit harder by federal changes than any other hospital in the state. In other words, the expenses were already growing at a rate that required a reliable revenue source.
Even setting the budget shocks above aside, HCMC faces three categories of structural operating deficits that grow every year. Hennepin County staff and this statement use conservative estimates to outline basic possibilities.
Uncompensated care is growing rapidly. In 2020, 6% of HCMC patients were self-pay (uninsured), and uncompensated care cost $40 million. By 2024, the self-pay rate had reached 8% with uncompensated care growing to $104 million.
Costs outpace reimbursements every year. Healthcare costs typically inflate at 5–8% annually, while reimbursements increase only 1–2%. County staff modeled a conservative 2% inflationary gap — the most conservative estimate they could responsibly use. Even at that floor, the difference between what care costs and what HCMC gets paid compounds every single year.
Critical equipment and capital investment have been deferred. A hospital the size of HCMC should invest approximately $50 million per year in replacing medical and IT equipment. The cash crisis has forced those purchases to be delayed. The campus spans more than 4 million square feet which is roughly 8 city blocks. Some of our buildings are over 100 years old. In just the last 16 months, the hospital experienced over 80 catastrophic infrastructure events, including flooding and HVAC failures. Deferred investment does not make costs disappear. Unfortunately, it only makes them larger and more impactful.
When HR1 hits, the math gets significantly worse (revenue replacement)
The federal legislation known as HR1 introduces two changes in coming years that will compound directly on top of the structural deficits above. In other words, in addition to seeking revenue due to growing expenses — anticipated federal changes result in the need to replace revenue at a rate that is mathematically not possible with property taxes.
To understand why these changes hit HCMC so hard, it helps to understand one key fact about HCMC's payor mix: Medicaid Managed Care is actually HCMC's best payor in terms of the percentage of costs it covers. That means HR1's changes to Medicaid reimbursement are not hitting a minor revenue stream, they are hitting the biggest part of HCMC's payor mix.
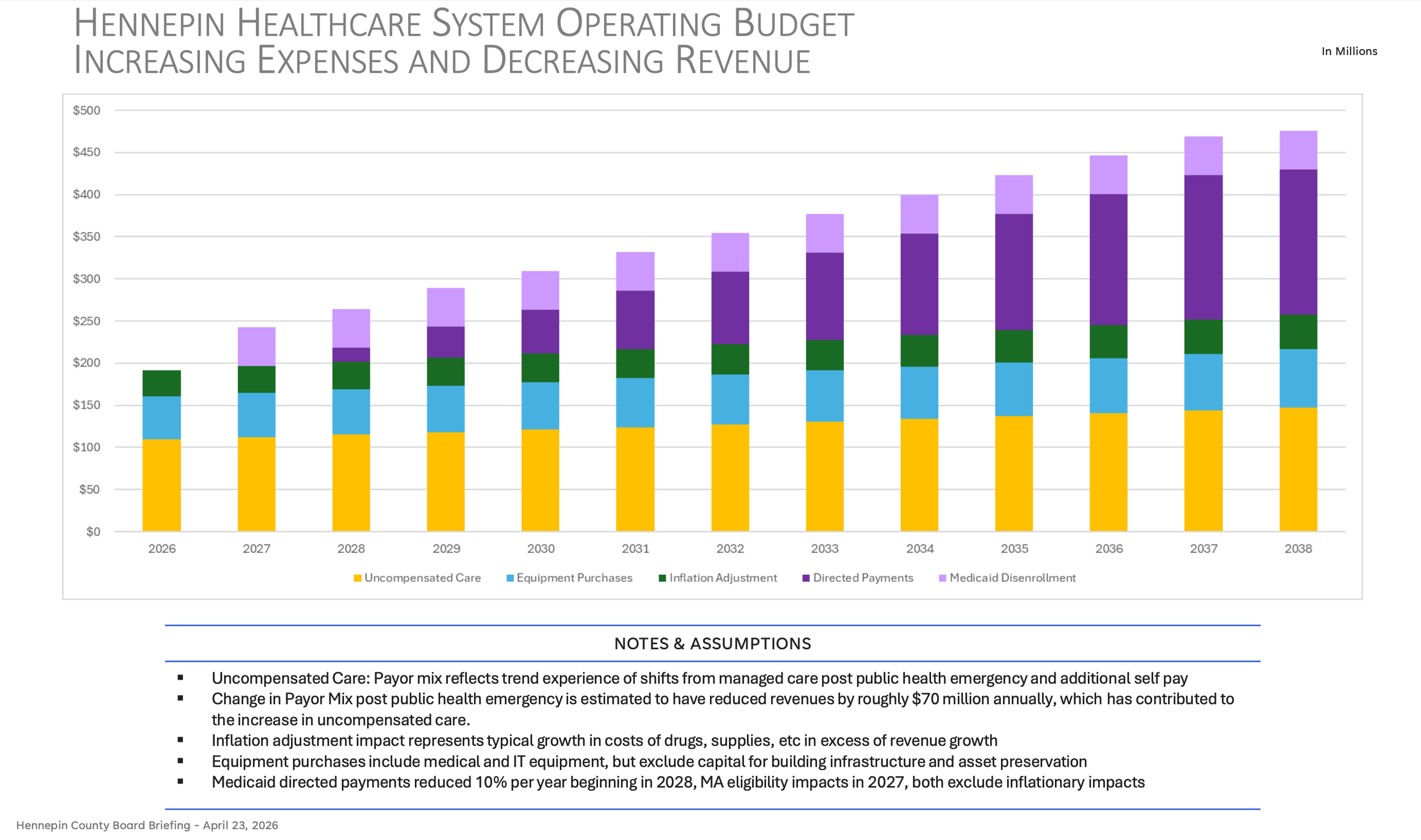
Hennepin County cannot property-tax a solution because the numbers are too big, which is why we urge the State to act now. The chart above shows the cumulative budget impact HCMC faces — in 2027, there’s nearly $200 million needed for growing expenses, and another $45 million for revenue replacement — and the untenable financial need grows and compounds each year.
The bottom three layers represent the growing expenses and structural deficits HCMC faces even without any federal changes — yellow (uncompensated care), blue (equipment), and green (inflation).
In 2030, growing expenses will exceed $200 million of need with no reliable revenue sources.
The top two purple layers show the revenue replacement needed due to HR1 impact arriving on top of growing expenses — light purple (Medicaid disenrollment beginning 2027), and dark purple (loss of directed payments beginning 2028).
In 2030, revenue replacement will exceed $100 million of need with no identified revenue sources.
In 2030, the total financial need exceeds $300 million of need with no proposed revenue sources.
In 2034, the total financial need will be approximately $400 million.
In 2038, the total financial need will be approximately $475 million.
These are not worst-case projections; the chart above represents the best estimates county staff could produce using the available modeling tools.
Medicaid disenrollment begins in 2027. HR1's new eligibility and work requirements and more frequent reauthorizations will cause thousands of patients to lose Medicaid coverage. Our neighbors, friends, and coworkers will lose health coverage but will still need care — many of whom will arrive at HCMC as self-pay clients, increasing our uncompensated care costs. County staff modeled a consistent year-over-year impact because the precise timeline of enrollment losses is difficult to project, but the total anticipated impact is significant and begins immediately in 2027.
Directed Medicaid payments phase out beginning in 2028. Directed payments currently allow Medicaid reimbursements to be set closer to commercial insurance rates. HR1 phases those out at 10% of value per year until reimbursements reach Medicare rates significantly lower than where they are currently set. Because Medicaid Managed Care is HCMC's strongest payor, this reduction hits harder here than at almost any other hospital in the state. This loss compounds annually as the rate steps down year after year.
$1.1 billion: the estimated cumulative loss to HCMC from directed pay reductions alone over the next decade.
$1.7 billion: the total estimated Medicaid-related revenue loss through 2038, developed using the Minnesota Hospital Association model and Department of Human Services estimates, with HCMC's share of Minnesota's Medicaid program applied.
Hennepin cannot mathematically property-tax a solution because the projected revenue losses are too large, which is why we are urging the Legislature to act on funding solutions that match the scale of financial need.
Why one-time State funding is not enough
Hennepin County has taken significant action toward saving HCMC. We have:
Raised property taxes for uncompensated care by 35.7%, bringing the annual contribution to $38 million.
Provided additional funding for capital projects, medical equipment, and IT hardware.
Made the significant move to have Hennepin County Commissioners serve as the interim HCMC Board since August 2025 — and had this vote not occurred, HCMC would likely have closed abruptly similar to other hospitals nationally.
Prioritized a single priority for the 2026 Legislative Session — identify reliable, non property-tax revenue source in order to save HCMC.
Every $11 million in additional property-tax support would require a 1% increase in the property tax levy. Hennepin residents cannot absorb the scale of increases that would be required to address the full gap HCMC needs — meaning, property taxes alone cannot save this hospital.
Any proposal for one-time or bridge funding does not resolve the fiscal cliffs approaching from HR1, nor does it address the years of deferred capital investment the campus requires because it cannot be borrowed against. It also places the hospital at risk of losing workers and accreditations.
What a sales tax would actually do — and why we need a sales tax specifically
Hennepin County presently has a 0.15% sales tax to fund the publicly-owned ballpark (Twins stadium), which is on track to retire early thanks to the County's strong financial management. Hennepin’s proposed solution to save HCMC is to modify this existing sales tax at an increased rate. An increased renewal of this sales-tax would:
Ensure the hospital is open for generations to come.
Close the structural operating gap from uncompensated care, inflation, and deferred equipment needs.
Fund critical capital investment in aging facilities. The campus requires $25–30 million annually just to keep buildings functional, before any modernization. In some cases, older buildings will need to be thoughtfully updated or reconfigured to reflect how modern healthcare is actually delivered and to meet current accreditation standards. The sales tax makes that possible without forcing crisis-driven decisions.
Invest in health workers. One weak recruiting cycle would affect staffing and care outcomes for nearly a decade. It costs over $70,000 to train a single nurse.
Protect HCMC's role training Minnesota's entire healthcare workforce — more than 50% of Minnesota physicians train at HCMC, including rural physicians, along with training programs across nursing, emergency medicine, pharmacy, and multiple other healthcare disciplines. The providers who will staff rural and suburban hospitals across the state for the next generation are being trained here right now.
It is also worth being direct about why a sales tax is the solution specifically. A sales tax is one of the only revenue sources that can be bonded against. That matters for a campus with $25–30 million in annual maintenance needs and buildings approaching 100 years of age. World-class care requires world-class infrastructure. Without the ability to borrow against a reliable revenue stream, large-scale capital projects, which improve operating efficiencies and meet current medical and accreditation standards, simply cannot be financed.
The state’s workforce is at stake
Without stable and ongoing revenue, the impact of a closure will reach far beyond HCMC. HCMC doesn’t just serve the patients that walk through its doors or are transported by its ambulances; it also trains Minnesota’s next generation of doctors, nurses, and paramedics. Greater Minnesota, along with rural areas across the country, is facing a shortage of healthcare workers that will only worsen in the coming years.
Rural legislators are hearing this directly from their local hospital administrators: they rely on HCMC to receive their most critical patients, and they rely on HCMC to train the providers who will keep rural hospitals staffed and open. The workforce pathways that serve outstate Minnesota runs through HCMC. Disrupting it here disrupts healthcare delivery across the entire state.
This is because 50% of the state’s doctors are trained at HCMC. HCMC is a crucial piece of the healthcare workforce in Minnesota, and its closure would reverberate across the state as fewer doctors are recruited to and set down roots in Minnesota, fewer paramedics are trained. Further, fewer nurses will develop the specialized skills that come only from caring for Minnesota's most complex, underserved, and critically ill patients, which will harm our statewide ability to provide care.
This is why saving HCMC isn’t just a Hennepin County issue, it’s a Minnesota issue. We have shown the math and now we need solutions that meet the scale of need, and urgently request the Legislature to allow Hennepin County to increase its sales tax for the health and well being of the entire upper Midwest region. A sales tax may not be the solution we want, but it is a workable solution during a time of immense dysfunction.
Will you take action to save our safety net?
Without dedicated revenue, the math does not work. The $1.7 billion revenue loss is coming. The structural deficits are real and growing. And the only public safety-net hospital in the upper Midwest, which sees 100,000 emergency patients per year, trains half of Minnesota's doctors and a significant share of its broader healthcare workforce, and provides care regardless of zip code or insurance status — cannot absorb what is coming without dedicated revenue.
We all have an HCMC connection. Maybe you were born there. Maybe your family received life-saving care there. HCMC has been there for all of us. Now it is time for us to be there for HCMC.
Today, I’m asking you to share why HCMC matters to you! Take a quick 15-second video and post it on socials. Share what HCMC means to you, your family, and your community. Learn more at CareForHCMC.org.